Publications IPH Magazine IPH Magazine, issue #14 How Architecture Has Influenced the Promotion of Hospital Hotel Services and Humanization

- Current Hospital Master Plan
- Architecture Regulations for Healthcare Facilities in Brazil
- How Hospital Rooms Went from Airy Temples to "Inhuman" Machines
- The healthcare hub
- Santa Casa de Misericórdia de São Paulo: A hospital architectural heritage
- How Architecture Has Influenced the Promotion of Hospital Hotel Services and Humanization
How Architecture Has Influenced the Promotion of Hospital Hotel Services and Humanization
Ana Augusta Blumer Salotti
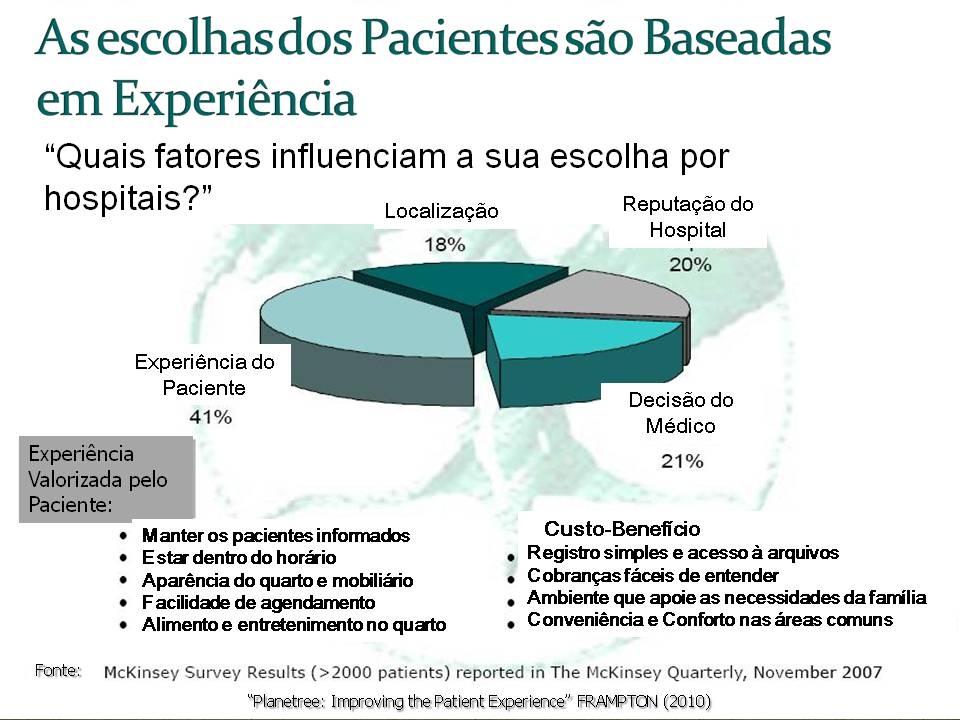
Among the experiences valued there are: keeping patients informed, being on time, quality of bedroom and furniture, facility to schedule, food and entertainment in the bedroom, simple admission and access to files, easy-to-understand charges, an ambiance that support the family's needs, convenience and comfort in the common areas. These subjects are deeply linked to issues like respect, amicability and support services that are to be provided by the hotel services department.
Hospital Hotel Services, Humanization and Quality: Putting the Current Scenario into Context
According to Frampton (2009), the aging of the generation whose behavior has been ruling the guidelines of economy for the past five decades, the baby boomers, is one of the factors that have directly influenced the soaring of the demand for health services and consequently the increased expectation of the consumer regarding his experience in health care.
Moreover, we have grown more aware of the importance of preventive medicine, encouraged by a longing for longevity, well-being and quality of life (Pilzer, 2002).
Frampton (2009) also states that unlimited access to health information enhanced by the internet has furthered more critical and demanding users. Therefore, the patient loses his submissiveness and resignation attitude in order to stand out for his rights, demanding a more outstanding course of treatment. Taraboulsi (2003) emphasizes the importance of hospital managers to see (and treat) patients as clients who want to be heard, respected and have their needs met. By stating that the health consumer is more aware and demanding than ever, Taraboulsi (2003) also highlights that the level of criticism and demands from them has skyrocketed.
From that assumption, every one attending a health facility is an opinion leader and henceforth a potential client. Therefore, the concept of client becomes wider, meaning not just the user of the service but also relatives, companions, friends and visitors; this new client has new indentified needs and gaps to be filled.
Bigger the Offer, Bigger the Competition
If on one hand the demand has soared, as well as users' demands, on the other so has the competition.
According to Maia and Gil (2008), the most relevant changes in the health system began in the 1970s when the movement to introduce capitalism within health services began, which brought forth the medical-hospital complex.
This movement had its origin when health professionals and investors saw in the group of inhabitants who were not being taken care of by the government (up to the 1930s the public services were exclusively focused on serving underprivileged people) a very attractive market niche. It was the inadequacy of the public system to provide for this population, so far deprived from high-quality services, which made this movement possible thus opening space for the institutionalization of public health.
The rapid process of doctors' and other professionals' employment, the growth of profitable private establishments, the plummet of the importance of philanthropic and charitable institutions that were ruling then and the slowly constitution of an entrepreneurial ideology within the health industry were key in the institutionalization of health. (Panorama Setorial, 1999)
Maia and Gil (2008) also affirm that the segment has experienced fast expansion and euphoria due to private networks valorization and the beginning of group medicine, through health operators and insurances. The writers say that until 1983 Golden Cross owned 95% of insurance and health care national market. The company started in 1971 and was the market leader until 1985 when the major commercial banks launched their health insurances (Las Casas, 1993).
Naturally, for the Brazilian health institutions to survive they needed to provide the high-quality and excellent services people were searching for.
Difficulties that Enhace Opportunities
Due to a bigger demand from users and bigger competition for service providers, two major tendencies egress:
- Hospital Hotel Services: aiming to meet the needs of clients (including patients, relatives, companions, friends and visitors) through amiable and hospitable services, besides introducing support services traditionally offered by hotels adapted and applied to the hospital reality, adding value and contributing for a better perception concerning the experience of hospitalization.
- Search for Quality: aiming to correct and improve services and processes; more efficiency and safety; economy and intelligence when using resources; and, above all, increase client's satisfaction through ongoing improvement heading to excellence.
Hospital Services: Care that is Noticed
Changes in architecture, social agenda, hotel services with doorman and concierge duly dressed and equipped to host the health client, paintings hanging on the wall, music, restaurant, piano-bar and musicians performing (piano and violin) give the impression of having the wrong address. When entering the lobby of some private hospitals, one might have the feeling of being at a five-star hotel. Gurneys, mass of health clients waiting to be seen, wheel chairs lining up, cold environment smelling like ether are scenes from the past. By embracing this innovation some hospitals are looking less like a hospital. (Taraboulsi 2003)
Detaching the hospital environment from a perception as cold, dark and hostile as the disease is one goal of hotel services in hospital. It has also been establishing as an irreversible tendency for hospital institutions that have realized that they must conquer loyal clients in order to survive.
According to Brandalise (2010), hotel services in hospitals are been used as a tool to strengthen the brand through attracting an outside public by promoting events and offering quality services to those living or working nearby.
At Hospital do Coração (HCor), in Paraíso, in the south of São Paulo, for instance, the dishes coming out of the kitchen are not at all jelly and unsalted rice soup. On the daily menu there are five types of salad, meat of every kind and even feijoada (pork, rice and black beans) in meals available not just to patients, companions and doctors but to anyone who wants. Brandalise (2010).
In the same article, Dr. Cláudio Lottenberg (doctor and president of the Sociedade Beneficente Israelita Brasileira Albert Einstein) highlights the importance of dissociate the hospital environment from the disease and when talking about the opening of the hospital's new auditorium he concludes his line of thought by stating that "Linking health and culture is something that must become ordinary. It is part of a wide understanding of what health means. (...) But it's certain that (the auditorium) will draw people to learn better about health-related issues and - why not? - to have fun". Brandalise (2010)
Boeger (2009) goes beyond when emphasizes the impact of hotel services in the experience of hospitalization. For patients and companions the way of treatment during the services provided are easier to notice than the investment made in high technology and in equipments and the outstanding technical performance of doctors.
Picture: Chart of Intensity in the Contact with the Client. Source: Boeger, 2009
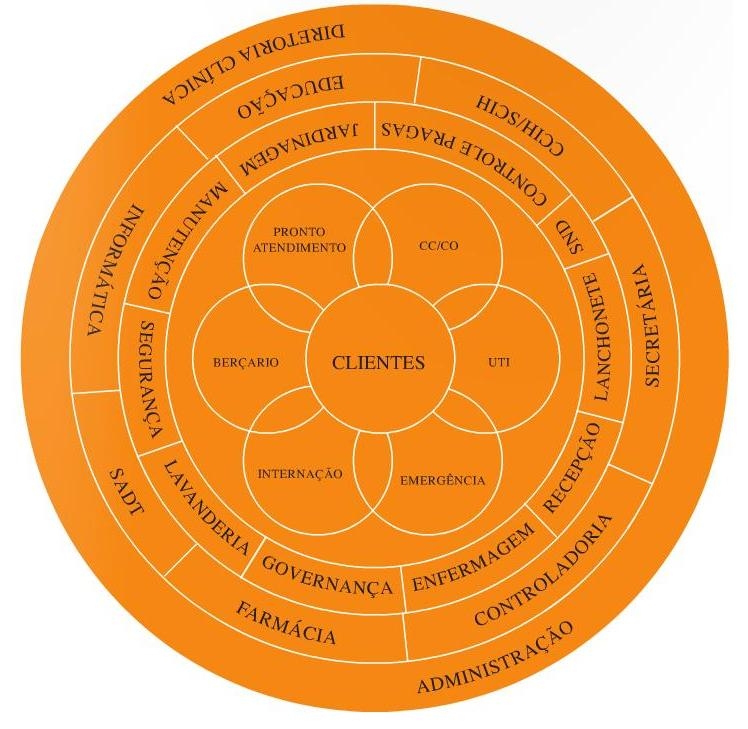
Therefore, depending on how each institution is managed, the cluster of hotel services may include:
- Gastronomy: nutrition and diet service combined with the creativity of chefs; room service; possibility to choose from other restaurants.
- Governance: laundry, hygiene, maintenance and gardening services, interior design and plague control.
- Security: estate security, surveillance, parking lot and entrance hall.
- Front Office and Hosting: reception; admission; hospitality (including a concierge service) and customer service or ombudsman.
The implementation of these services within hospitals for the past decade has been groundbreaking; nonetheless, there is still a label that comes along the concept: hotels are usually associated with luxury, hospitality to well-being and Hospital Hotel Services to private hospitals.
However, when the concepts hotel services and hospitality are fully understood, the fastest association should be: sheltering, education, politeness and prone to serve. According to Boeger (2011), hospitality is connected to pre-established attitudes, which means: behaviors that depend on people rather than exclusively on resources to be implemented.
In order to better illustrate the concept of Hospital Hotel Services linked to hospitality, Gomes (apud Boeger, 2011) emphasizes that the core goal of the field is "to demonstrate to the client that he is in the center of everything, that he is the institution's biggest concern, that the hospital is on his side to take care of his physical, mental and emotional well-being, helping him to overcome this detour in his life".
This is the origin of the "hospital humanization" concept, enhancing the need to include actions that respect and value the health client as a human being as an institutional culture and not just as an implementation of isolated actions and individual effort.
As a result, we may conclude that hotel services in hospitals must have the behavioral interface profoundly connected to the institutions' mission, vision and values. If not, the cluster forming this department ends up as a group of support and convenience services offered to patients and companions, not adding any value of uniqueness despite easiness.
Health Institution: Where Is your Focus?
During his lecture at the ExpoManagement 2007, Michael Porter forcefully warned the audience to the importance of patient-centered care: "Nowadays, we have a scenario in which hospitals want to offer everything, competing for nothing. As long as the focus is not on the patient, they will all keep on losing" (Source: http://www.saudebusinessweb.com.br/noticias/index.asp?cod=43302 read in February 2011).
Still, to meet patients' and clients' needs it is necessary to know what they want and how they perceive the service received.
Therefore, all it takes is to listen to what they are saying.
Focus on the Patient = Security
The general manager of a multinational-chain hotel in São Paulo (2011) believes that the three success-leading factors according to clients are: consistency, quality and security.
According to the interviewee "(...) the same procedures are undertaken here, in the US or in Asia... so the guest is never taken by surprise with the quality of the company, which is worldwide standard". Hence, the services provided convey reliance, not only attracting clients, but making them loyal to your brand.
This is not a need just within lodging services: much more important than a safe place that provides services in a consistent manner and with quality to spend a certain amount of time for pleasure or work, is the place people trust to take care of their health and their lives.
A research undertaken by the Joint Commission Journal on Quality and Patient Safety indicates that patients see a defective service (or week, poor) as not safe: 22% from 193 patients recorded going through a "recent unsafe experience", among which only 3% concern medical incidents or near mistake. More than half of the events were classified as "incidents in the quality of services" such as:
- 30% concerning waiting and delays;
- 21% concerning lack of communication;
- 12% concerning environment issues.
We may understand, consequently, that "Patients may perceive these inconveniences as a warning against the whole treatment process". (Source: Patient Reported Safety and Quality of Care in Outpatient Oncology - Joint Commission Journal on Quality and Patient Safety; 33:2, 2007).
In an article published by the United States National Medicine Library, the hypothesis that patients who reportedly receive low quality services would be more prone to a higher risk of suffering medical mistake or adverse events was confirmed as shown in the conclusion: "Patients that report incidents in the quality of the services can help identifying risks to the patient's safety." (Source: "Do Medical Inpatients Who Report Poor Service Quality Experience More Adverse Events and Medical Errors?" Med Care. 2008 Feb; 46(2): 224-228 http://www.ncbi.nlm.nih.gov/pubmed/18219252 read on March 25 2011).
"It is necessary a course of care that focuses on the patient and embraces effective communication as well as technical abilities to reach safety and quality assistance", so conclude the specialists from the Institute of Medicine. (Source: Institute of Medicine, Preventing Medication Errors: Planetree, Improving Patient Experience, Frampton 2010).
The writers Baker and Bank (2008) have broaden our understanding concerning clients' perception regarding services offered according to their dissatisfaction by reading true complaints resulting from hospital services, home care and clinics served by the Ombudsman or Customer Care. That was the starting point to select the "101 Most Common Complaints About Health Care", (sentence that gives the book its name).
Taking into account the reason for the complaints, the conclusion enhances the data aforementioned, which means, more than 60% of clients' dissatisfaction concern:
- Quality (of services, treatment, waiting time, lack of attention or communication);
- Ambiance (infrastructure, comfort and autonomy);
- Access (reception, accessibility and sheltering).
Brady and Conway (apud Frampton and Charmel 2009) emphasize the importance of considering patients as partners to succeed. "The efforts to engage patients as partners in their safety must be based on a patient-centered approach that:
- Sees the patient as a partner;
- Listens to and respects their opinion;
- Foresees and meets their needs,
- And, simultaneously, cares for the staff, so it can provide a more effective assistance."
The writers conclude explaining that safety against non-intentional risk is a basic need of all patients and that is not possible to be truly patient-centered without being safe. At the same time, it is not possible to be safe without being patient-centered.
Support Services: Moment of Truth
Hotel services, whether the traditional ones or in hospitals, have as the most important product offered its services, which means: intangible assets that are evaluated according to the user experience that is called "Moment of Truth".
According to Carlzon (1987), the term Moment of Truth covers the period of time during which the client interacts with the company, its employees and the physical environment, allowing them a perception of the quality of the service (Source: http://www.cullencia.com.br/archives/206 read on March 21, 2011).
Therefore, these moments include the whole experience of the client with the service offered even prior to his arrival at the institution: from scheduling an appointment with the physician or a surgery over the phone; his arrival, admission up to the moment he is discharged and leaves the hospital.
During such moments, hostility, indifference, coldness or disrespect are as noticeable as hospitality and humanization, whether it is in the care and kindness of the nurse or in the attitude of the valet upon receiving or returning the patient's car. Thus it explains how important it is to consider the hospital staff as a whole as care takers, as praised by Planetree, a model of quality management. (Frampton and Charmel, 2009).
The services offered are not always valued by the client, which is a problem for the quality of the services offered and for the image of the institution. As said before, in a hospital, services are consumed and provided at the same time. How intense and deep the contact between staff and clients may be are relevant factors for the perception of these services. (Boeger, 2009)
Depening the importance of support services provided for the construction of a favorable hospital experience, the results from a research undertaken by McKinsey (2007) show that when choosing a hospital 41% of the patients are influenced by their experiences.
Graphic: "Factors that influence the patient's choice for a hospital"
Source: McKinsey (2007) extracted from the presentation "Planetree: Improving the Patient Experience" Frampton 2010 (free adaptation from the writer of this paper).
Among the experiences valued there are: keeping patients informed, being on time, quality of bedroom and furniture, facility to schedule, food and entertainment in the bedroom, simple admission and access to files, easy-to-understand charges, an ambiance that support the family's needs, convenience and comfort in the common areas. These subjects are deeply linked to issues like respect, amicability and support services that are to be provided by the hotel services department.
The medical assistance is as important as all the services that support both the patients' care and the patients' and their companions' comfort, therefore: it is key to be careful with focus on patient, safety, quality and support services are deeply connected.
Wherefore, the transformations concerning hospital architecture begin with queries regarding these priorities:
- How to provide more autonomy to the patient whenever possible?
- How to provide better opportunities of human interaction in every level (patients and relatives; patients and multidisciplinary team; relatives and team and so on.
- How to enhance privacy to internal and external clients?
- How to offer coziness and comfort within environments?
Quality Model Focused on Humanization
Unlike the other quality models, the Planetree is based on a course of treatment that focuses on the patient and considers his perspective. Since it is a philosophy based on institutional and behavioral cultural changes, rather than on processes and physical structure, the road to accomplish this recognition is called affiliation. After certification, the affiliate hospital becomes a "Designated Planetree Hospital".
When questioned about the major differences between Planetree and other accreditation organizations, Alff (2011), who was responsible for implementing the Joint Commission for about fifteen years, places Planetree as an organization that brings together its affiliates as partners and works to take the institutions from where they are to where they want to be. While the Joint Commission has very specific criteria to be met (thus developing a consultancy with judging character), Planetree is a more customized consultancy with a collaborative profile. Alff (2011) also says that the model recognizes that there are numerous ways of creating a positive environment for patients depending on what they wish for. For that, it is necessary to analyze and respect the uniqueness of each country, the profile of patients treated and the weak points that must be improved.
Planetree was founded by Mrs. Angelica Thieriot after she had experienced a traumatic period of hospitalization. During which the lack of information, impersonality, coldness and the darkness of the spaces enhanced her insecurity, anxiety and fear. After surviving this experience, she left the hospital strongly determined to change the way medical care is delivered, defending the rights and establishing herself as a spokesperson of all patients.
She then received the help of a multidisciplinary team formed by renowned and visionary professionals among doctors, nurses, educators, architects, interior designers, nutritionists and financial managers, committed to create a truly new care model in the hospital industry.
Founded in 1978, this non-profit organization is named after the Platanus tree (also known as Plane tree), under which Hippocrates used to teach. One of the guidelines upon which the philosophy of this model was based on was Hippocrates' lessons that emphasized the importance of listening to the patients.
The refocus of medical attention on the patient, considering the influence of his personal beliefs, wishes, fear and yearnings in the treatment as a whole is covered by the authors of the book "Planetree, Putting Patients First" as a key factor to generate contributions for the healing and recovering processes, being directly related to the concept of embracing hotel services in the hospitals, as well as the demystification of admission: a hospital that does not look and smell like a hospital is the goal of the model and is the reason why the whole team engaged and is committed to its creation.
According to Charmel and Frampton (2008), the patient-centered care may be defined as a health assistance scenario in which patients are encouraged to have autonomy through active involvement in their own treatment; it takes place in a pleasant space and makes available a dedicated team that meets the physical, emotional and spiritual needs of patients. For a model to be considered a patient-centered one, it must cover the following requirements:
- An organizational culture that encourages the team to be sensitive to the needs of the patient during his stay in the hospital;
- An architectonic and interior design that gives a homemade touch and encourages the patient's mobility, the involvement of the family in the process and a space addressed to both solitude and social activities;
- Emphasis on the education of patients and relatives;
- Recognizing nutrition as a whole part of health as well as a source of pleasure, comfort and familiarity;
- Supporting the involvement of family members in the treatment, care and assistance process.
(Source: "Building the Business Case for Patient-Centered Care", Charmel and Frampton, 2008)
Summing up, the designate institutions are encouraged to change the way hospitalization and hospitals are perceived by patients and their relatives.
The bases and pillars of this philosophy can be defined when three simple questions are answered by the patients: "have we helped you to live your life with dignity and reach ideal health?"; "Have we helped you to obtain the cure at the highest level possible?"; "Have we helped you grow in every significant aspect, whoever you are?"
According to Charmel and Frampton (2008), "Nowadays, the patient-centered care have been embraced by the most influent health service providers, developers of new policies, regulatory agencies, researchers and founders". This remarkable progress may be due to a study from the Institute of Medicine from 2001 that identifies the focus on the patient-centered care as one of the six interrelated factors that constitute high quality assistance.
This has strengthened the approach of the concept not only as a mean to create a more attractive experience for the patient but also as a fundamental practice to provide high quality care.
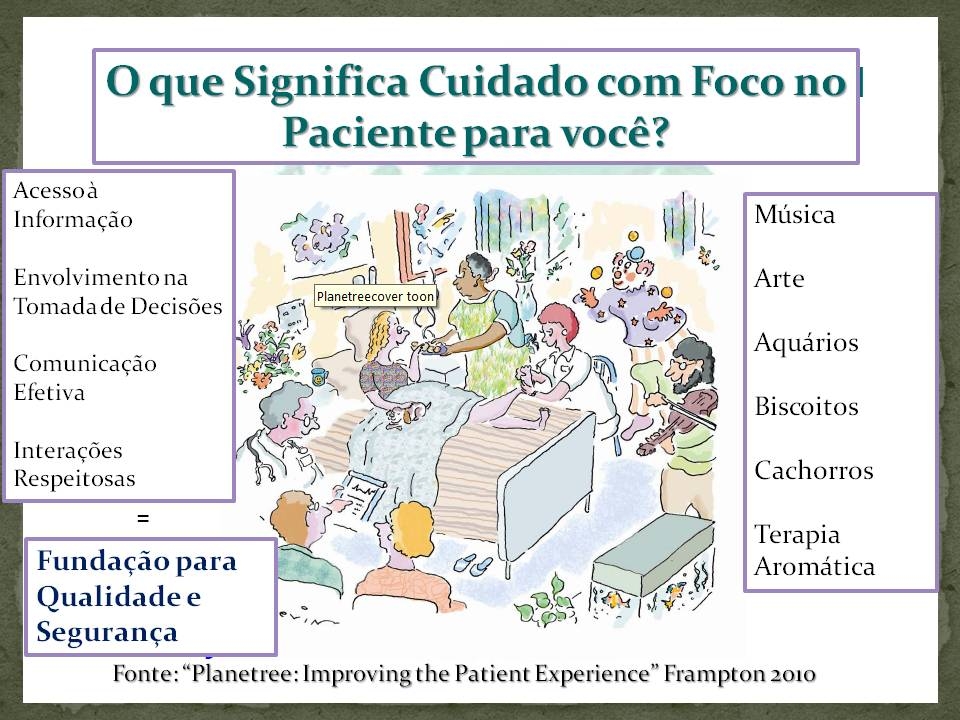
Picture 2: What does Patient-Centered Care Mean to You?
Source: Frampton, 2010 (adapted by the author of this paper)
This is how the model here presented combines the concept of hotel services and quality as one whole part of assistance, impacting not only the before, during and after admission that relates just to the perception of the treatment and the hospitalization experience, but also they also contribute, specially and effectively, to the development of an environment appropriate and favorable to the healing process and patient's recovery, patients that are now seen and recognized as people (in the whole, and not considered only according to his disease or clinic condition). They are people who bring along beliefs, values and expectations, besides the fundamental power that can define the survival and health of organizations: the power to decide between this or that institution, depending on how certain needs and expectations are received and met.
Daring to go even further, Planetree defends, in one of its most important principles, the importance of environments as allies to allow the patient's healing and recovery.
Concluding, we may comprehend the influence of Hospital Architecture in promoting a safer assistance, more dignified and humane for patients, companions and relatives, as well as for the numerous professionals working in hospitals.
Bibliography
ANDRADE, SANTOS e SAMMOUR. Contribuição da Hotelaria Hospitalar para os Processos de Acreditação de Instituições de Saúde. São Paulo, Instituto de Ensino e Pesquisa do Hospital Albert Einstein, 2008.
BAKER, Susan e BANK, Leslie. "I'm Sorry to Hear That..." Real Life Responses to Patients' 101 Most Common Complaints About Health Care. Connecticut, Fire Starter Publishing, 2008.
BOEGER, Marcelo. Lecture at the Post-Graduation Course in Hospital Services. São Paulo, Instituto de Ensino e Pesquisa Hospital Israelita Albert Einstein, Março 2010.
______. Gestão em Hospitalidade e Humanização. São Paulo, Editora Senac, 2009.
______. Hotelaria Hospitalar, Manuais de Especialização. São Paulo, Editora Manole/Sociedade Brasileira Beneficente Israelita Brasileira Albert Einstein, 2011.
BRANDALISE, Vitor Hugo. Hospitais Viram Opção De Lazer e Restaurante. São Paulo, Jornal O Estado de São Paulo, October 5 2010.
CABRERA, Luiz Carlos. Inovação e Liberdade. São Paulo, revista Você S/A, Ed. Abril, September 2010.
CALEGARI, Rita. Humanização, Uma Questão de Atitude. São Paulo, Lecture given on October 5 2010, at the IX Fórum de Hotelaria Hospitalar at the Centro de Convenções Rebouças.
CARNEGIE, Dale. Como Fazer Amigos e Influenciar Pessoas. São Paulo, Companhia Editora Nacional, 2003, 51ª edição.
CHARMEL, Patrick e FRAMPTON, Susan. Building the Business Case for Patient-Centered Care. Illinois, revista Healthcare Financial Management, 2008.
FOLGATO, Marisa. Cumplicidade e Carinho. São Paulo, Revista da Abrale, March/ April / May 2010.
FRAMPTON, Susan e CHARMEL, Patrick. Putting Patients First, Best Practices in Patient-Centered Care Planetree. San Francisco (EUA), Jossey Bass 2009 (second edition).
FRAMPTON, Susan. Planetree, Improving the Patient Experience. Connecticut, Apresentação em Power Point cedida por Marie Sullivan do Planetree in October 2010.
HANNOCK, T. Seeing the Vision, Defining Your Role KRUPSKI, T. among others. Spirituality Influences Health Related Quality of Life. In.: Men with Prostate Cancer Psychooncology. Health Care Forum Journal, from May to June 1993.
INSTITUTE OF MEDICINE. Crossing The Quality Chasm, A New Health System for the 21st Century Committee on Quality of Health Care in America, National Academy Press, Washington, D.C.
ISAAC, Humberto Jorge. Saúde como Prioridade. São Paulo, revista Universo Unimed, January / February 2011.
(The) Joint Commission. What did the Doctor Say? Improving Health Literacy to Protect Patient Safety Chicago, The Joint Commission, February 2007. Read on December 17 2007.
KRUPSKI, T. e outros. Spirituality Influences Health Related Quality of Life in Men with Prostate Cancer. California, Psychooncology, 2006.
LAS CASAS, A.L. Marketing: Conceitos Exercícios Casos. São Paulo: Atlas, 1993.
LEPORE, Michael. Understanding Why Caregivers Do What They Do. Connecticut, Planetalk magazine, February 2011.
MAIA, Anselmo e GIL, Antonio. Miopia em Marketing no Segmento Hospitalar do Brasil, MTC Desenvolvimento Empresarial 2, 2008.
MASETTI, Morgana. Soluções de Palhaços - Transformações na Realidade Hospitalar. São Paulo, Palas Athena, 1998.
MCCAUL, K. D., e MALOTT, J. M. Distraction Coping with Pain, Psycological Bulletin, 1984.
MCGAHEY-OAKLAND, P. R., LIEDER, H. S., YOUNG, A. e JEFFERSON, L.S. Journal of Pediatric Health Care, 2007.
MELLO, Kátia. Vida após o Câncer. São Paulo, jornal Folha Universal Edição 969, October 2010.
MIRAMONTES, Andrea. A Fórmula da Felicidade, jornal Folha Universal Edição 965, October 2010.
MUSSAK, Eugenio. Encontre sua Filosofia. São Paulo, revista Você S/A, Abril, September 2010.
PAVAN, Cleusa. Política Nacional de Humanização da Atenção e Gestão do SUS. São Paulo, lecture given on March 18, 2011, at Hospital Emílio Ribas.
PILZER, Paul Zane. The New Wellness Revolution: How to Make a Fortune in the Next Trillion Dollar Industry. Nova Jersey, John Wiley and Sons, Inc. Roboken, 2002.
RAGNESKOG, H. e outros. Dinner Music for Demental Patients: Analysis of Video-Recorded Observations. Clinical Nursing Research, 1996.
ROSSO, Fabrízio. Gestão ou Indigestão de Pessoas? Manual de Sobrevivência para RH na área da Saúde. São Paulo, Edições Loyola, 2003.
SENDIN, Tatiana. A Era dos Valores. São Paulo, revista Você RH, Abril, July / August 2010.
STANDLEY, J. Clinical Applications of Music and Chemotherapy: The Effects on Nausea and Emesis. Music Therapy Perspectives, 1992.
SZKLARZ, Eduardo. Abrace o Colega ao Lado. São Paulo, revista Super Interessante, May 2010.
TARABOULSI, Fadi Antoine. Administração em Hotelaria Hospitalar. São Paulo, Editora Atlas S.A., 2003.
(The) Joint Commission. National Patient Safety Goals The Joint Commission, fevereiro de 2007. Read on December 17 2007.
TOZZI, Elisa e BASTOS, Thiago. Seja Feliz. São Paulo, revista Você S/A, Ed. Abril, September 2010, edição 147.
TRESOLINI, C. P., e PEW-FETZER. Task Force. Health Professions Education and Relationship-Centered Care São Franciso, Pew Health Professions Commission, 1994.
ULRICH, R. S. Biophilic. Theory and Research for Health Design. In.: S. Kellert, J. Herwagen, and M. Mador, Biophilic Design: Theory, Science, and Practice. Nova York, Wiley, 2008.
________. View Through a Window May Influence Recovery from Surgery. Science, 1984.
WALSH, S. M. MARTIN, S. C. e SCMIDT, L. A. Testing the Efficacy of a Creative-Arts-Intervention with Family Caregivers of Patients with Cancer. Journal of Nursing Scholarship, 2004.
WEIS, Charmaine. When our Patients Talk, We Listen. Connecticut, revista Planetalk, February 2011.
ZANOVELLO, Ana Lúcia. Lecture Given at the Post-Graduation Course in Hospital Hotel Services São Paulo, Instituto de Ensino e Pesquisa Hospital Israelita Albert Einstein, August, 2010.
Webgraphy
Canadian Accreditation, read in March, 2011
BACH, Peter, Md. The Doctor Who Knew Too Much Well Blog, The New York Times, read on March 4, 2011
Users Right Letter (PNH) read on March, 2011
CQH, read in March, 2011
Dictionary, used on 27 March, 2011
Do Medical Inpatients Who Report Poor Service Quality experience More Adverse Events and Medical Errors? Med Care. 2008, read on March 2011
DUO, Thaia Unimeds apresenta resultado da verticalização, Saúde Business Web, read on March 2011
Joint Commission, read on March 2011
MARTINS, Ana Paula Competição Baseada em Valor é a Saída para a Saúde Saúde Business Web, read in February, 2011
Momentos da Verdade, read on March 21, 2011
ONA, read on March 2011
PNAS High income improves evaluation of life but not emotional well-being,
read on March 30, 2011
Portal Humaniza, read on March 2011
Política Nacional de Humanização, read on March 2011
Portal Saúde (Ministério da Saúde), read on March 2011
Reitora e Professora de economia e relações públicas da Escola Woodrow Wilson, Christina Paxson, read on March 30, 2011
Verticalização da Saúde Suplementar, Saúde Business Web, read in March 2011
Videos
Animal Therapy and Spirituality, the Importance of Inner Resources, watched in March, 2011
Marília Gabriela Interview Dra. Nise Yamaguchi, broadcasted on November 14, 2010 (watched in March, 2011)
Sharp Coronado Hospital, watched in October, 2010
Share




Send by e-mail: