Publications IPH Magazine Revista IPH Nº17 COVID-19 pandemic and the trends in healthcare design: insights from the "Decalogue for Resilient Hospitals"
- IPH Magazine #17
- COVID-19 pandemic and the trends in healthcare design: insights from the "Decalogue for Resilient Hospitals"
- Healthcare closer to people: A qualitative study of a Swedish reform on healthcare delivery
- Spatial flexibility and extensibility in hospitals designed by João Filgueiras Lima
- Design Insights from a Research Initiative on Ambulatory Surgery Operating Rooms in the U.S.
- A study on the development of the concept growth and change on hospital architecture in Japan
- A study on hospital infection control through architecture in 1980: Chapecó Regional Hospital case study
- Natural ventilation for hospitalization environments: historical aspects
- Hospital architecture and its propositions for beginners and experts
COVID-19 pandemic and the trends in healthcare design: insights from the "Decalogue for Resilient Hospitals"
Stefano Capolongo, Andrea Brambilla and Marco Gola - Instituto Politecnico di Milano, Italy

Abstract.
The COVID-19 pandemic has stressed the healthcare systems at global scale with specific regards to hospital organizations and facilities. The surge in infections and the huge number of critically ill patients has tested the flexibility of architectures for health forcing organizations to quickly adapt and exploit ad-hoc emergency solutions.
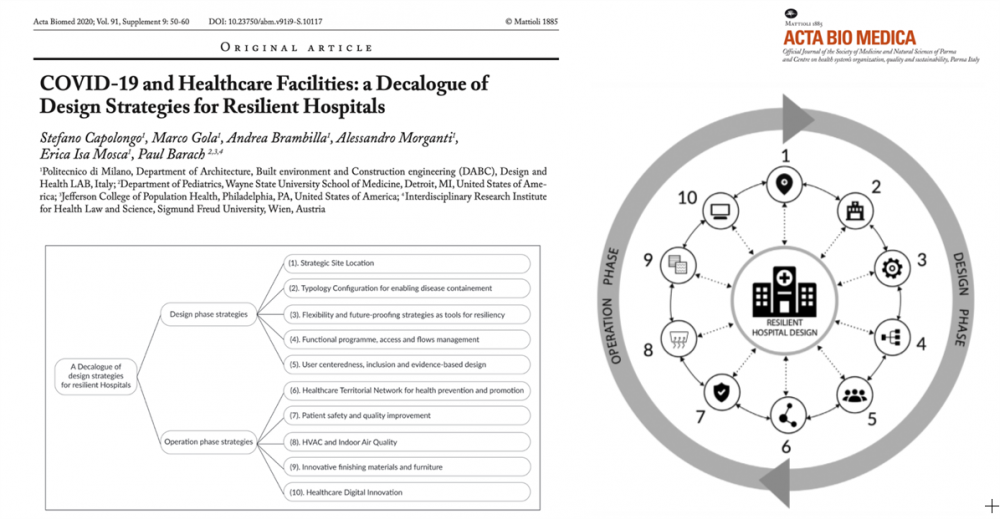
The paper proposes insights from the "Decalogue for Resilient Hospitals" which includes a series of design strategies and considerations applicable both to new hospitals and to the refurbishment of existing hospitals. The proposed strategies involve: 1) Strategic Site Location; 2) Typology Configuration; 3) Flexibility; 4) Functional program; 5) User-centeredness; 6) Healthcare network on the territory; 7) Patient safety; 8) HVAC and indoor air quality; 9) Innovative finishing materials and furniture; 10) Healthcare digital innovation. The COVID-19 pandemic disrupted healthcare operations and accelerated the processes of innovation and transformation. The incorporation of future-proofing design and operational strategies into new or refurbishment projects can enable the achievement of resilient hospital facilities.
Key words:
COVID-19; Hospital; flexibility; resilience; digital innovation; patient safety.
COVID-19 impact on healthcare systems
The COVID-19 virus is creating unexpected stresses on architectures for health and critical care systems. The rate of infections and critically ill hospitalized patients reached unprecedented levels.
Hospitals play a crucial role within the healthcare system in providing essential medical care to all the community, particularly during an emergency. In general, they are complex and vulnerable institutions, dependent on critical external support and supply lines which operate at a very high rate and capacity.
Even a modest rise in admission volume during a relatively short period of time can overwhelm a hospital beyond its functional reserve. The COVID-19 pandemic has stressed critical support service clusters and interrupted supply chains along with medical staff shortages and communications challenges (WHO, 2020). Healthcare facilities struggled to adequately respond to an unprecedented demand for emergency care and Intensive Care Units (ICUs) for infectious diseases. The need of COVID-19 beds in acute care departments globally surged, forcing healing settings to adopt contingency capacity strategies such as adaptations to medical care spaces, staffing constraints, and supply shortages in order to increase their overall capacity.
The emergency underlined all the existing structural, technological and organizational challenges of worn-out and obsolete hospitals. In fact, they were seen to undermine resiliency and efficiency in tackling rapid epidemiological, economic and social changes that was necessary for addressing the COVID-19 surge. In addition, starting in the short term, healthcare systems will face two collateral issues: the growing delay of ordinary healthcare procedures (i.e. delay in cancer procedures, operations, etc.) and the physical and mental stress caused by the critical situation to healthcare workforce (VV.AA., 2020; Barach et al., 2020).
In order to overcome the worldwide saturation of spaces within existing hospitals, two main strategies have been exploited:
- starting from the example of Wuhan in China, that built an emergency hospital in 10 days, the whole world has taken the challenge to build several temporary structures to help support the great demand for beds for COVID-19 patients. Facilities designed to support the care of many patients, on a 25.000 square meters of prefabricated blocks were undertaken as the symbol of how innovation in construction field can impact on healthcare processes. Countless temporary solutions such as containers, inflatable systems, tent structures, modules, partition panels, ships have been proposed by designers around the world, such as the CURA (Connected Units for Respiratory Ailments), the open source project by Carlo Ratti Associates (Italy) or the 68 beds and 10 ICU beds at the East Meadow in Central Park in New York City (USA);
- another strategy regarded the transformation of non-sanitary building typologies, unused during the pandemic, such as re-tooled trade centers, airports, schools, etc. Several studies developed by designers resulted in conceptual works to convert schools or hotels into temporary healthcare spaces in 14 days or less. In addition, a taskforce set up by the American Institute of Architects (AIA, 2020) provided a planning tool to quickly identify suitable buildings for patient care. Examples can be found in the transformation of the Exhibition Center "Fiera Milano" in Milan (Italy) and ExCel Center in London (UK) and where also important transformations on HVAC systems were done; in any case, these examples have several limitations such as a limited capacity for surgery or high level diagnostics, lack of specialized support services and being distant from the core hospital.
The challenge of healthcare facilities
While outside the hospital temporary structures emerged, within the existing facilities the healthcare organizations had to deal with two emerging issues:
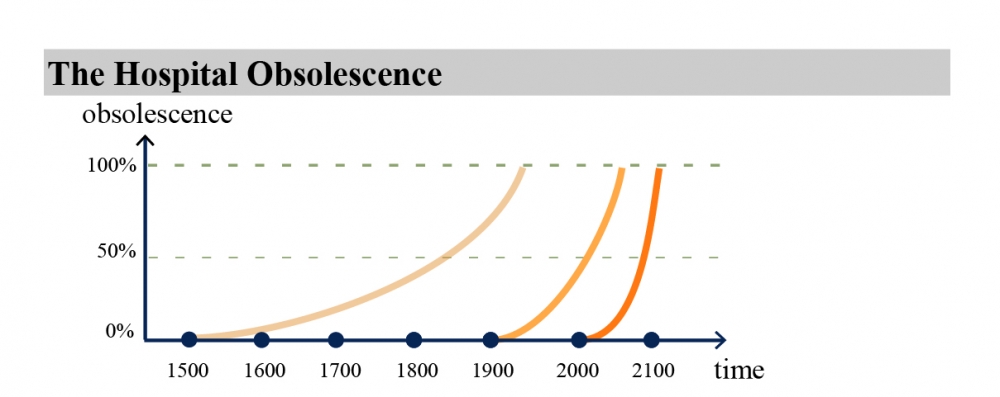
- treating patients with severe symptoms while reducing the spread of the virus among users and medical staff. In order to deal with the first aspect, there was a rapid conversion of different facilities such as hotels, trade centers, airports, etc. into new hospital spaces, revealing a series of operational and safety difficulties that can be summarized in the structural impossibility to separate a critical care component (such as ICUs) from the rest of the hospital. Therefore, a large part of the COVID-19 areas have been designed in proximity with ad-hoc and extremely varied solutions according to the needs of the hospital, department or ward. The lack of a common comprehensive strategy is not only linked to the complexity of the emergency, but especially to the high complexity and highly variable hospital infrastructures. In fact, in terms of dimensions, number of users and volume of activities, the hospital is more similar to a city within a city characterized by stratifications of service networks distributed in indoor and outdoor. The general state of obsolescence and rigidity of healthcare has greatly contributed to the management and organizational challenges of this particular pandemic in several countries. Hospitals were forced to adopt several cross-cutting strategies including the creation of:
- creating dedicated spaces for donning and doffing of personal protective equipment (PPE) decontamination areas for healthcare workers; new spaces with prefabricated technologies;
- buffer areas between wards, the division between contaminated and non-contaminated areas, the transformation of acute care spaces (i.e. already equipped with advanced systems such suction, oxygen, negative pressure, etc.) starting from operating theatres;
- core and shell empty environments at disposal (so-called "lung" spaces) to be equipped for emergencies or also unused area, gyms, car parks or congress centers;
- the other challenge faced by hospitals is the virus containment. The lack of validated data and evidence-based protocols forced each hospital to develop ad hoc solutions sometimes based on models of prior epidemics caused by viruses such as SARS in 2003 and Ebola in 2012, or bacterial epidemics such as Tuberculosis. Coping with these highly contagious episodes required applying strict infection control protocols in the distribution areas, at key thresholds such as entrances to better manage the flows of medical staff who can infect themselves, and as a consequence other workers and users.
Figure 1. Hospitals obsolescence during the centuries. Figure taken from Capolongo (2012).
A Decalogue for resilient hospitals
Starting from these general considerations, the paper provide insights for the future healthcare architecture in terms of a Decalogue of strategies for new perspectives in healthcare design. This work was promoted by the Department of Architecture, Built environment and Construction engineering of Politecnico di Milano (Italy) as an observatory on the best practices for resilient healthcare facilities.
This approach will support in responding to the needs for critical care capacity applicable both to new hospitals and to the refurbishment of existing hospitals to provide a clearer and more coordinated response for future healthcare emergencies (Capolongo et al., 2020).
The architectures for health of the future should be more and more resilient to changes and capable of protecting different users' health and tackling the transforming social, environmental, economic, and epidemiological needs of the context in which they are located. In the previous months, a comparative matrix has been structured in order to merge the strategies derived from the data and case studies collection. Two areas of improvement have been investigated:
1) strategies 1, 2, 3, 4 and 5 that can be implemented during the design phase;
2) strategies 6, 7, 8, 9 and 10 that can instead be achieved during the operation phase.
Figure 2. Outcomes of the "Decalogue for Resilient Hospitals". Taken from Capolongo et al. (2020).
1. Strategic Site Location
In the urban context, the hospital has a strategic role for different factors, such as the accommodation of a wide and diverse amount of users and visitors, the relevant building dimension and the economic supply chain. For this reason, hospitals' site selection is a crucial topic in planning decision processes that affects the social, environmental, and economic sustainability of healthcare structures and the efficiency of the service (Dell'Ovo et al., 2018).
In recent years, hospital trends have highlighted the importance of localization in urban areas, however past and ongoing experiences, especially in relation to an infectious epidemic, are challenging this trend. In fact, the capability of changing functional areas or spreading them outside, has been often limited due to the lack of flexibility expansion related to the hospitals' location in dense city center. Learning from the management of previous pandemics, the localization of the post-COVID-19 hospitals to the city boundaries can guarantee both the limitation of flows outside urban areas, containing possible risks of contagion in high-density urban centers and the accessibility.
At the same time, a correct strategic location represents an opportunity for spreading in areas close to the healthcare facility. On the other hand, central areas should preferably host territorial facilities able to provide: health services at the first level, prevention and health promotion at the neighborhood scale (Miedema et al., 2019).
2. Typology Configuration for Enabling Disease Containment
Nowadays, trends on hospital's typology are mainly characterized by horizontal configurations. In emergency state, this setting ensures the possibility to organize areas without constraining the entire distribution systems (Capolongo et al., 2019). In order to provide an effective emergency management, treatment areas for contaminated and infected patients to be isolated through a clear separation of flows, cross-contaminations should be avoided through the appropriate usage of dedicated vertical and horizontal connections for diverse areas. Therefore, a hybrid typological configuration, characterized by a main structure connected to support pavilions, might represent a strategic solution, with dedicated accesses for emergency and logistics vehicles.
In case of infectious emergency, the independence of the buildings or the availability of autonomous internal units, allows to separate different functional areas from the rest of the system, without ordinary activities interruption. Providing outdoor spaces around the hospital is also suitable for hosting additional temporary structures such as tents, tensile structures or other modular solutions, which guarantee the connection to the hospital and the relationship to driveways for ambulances and logistics vehicles.
3. Flexibility and Resiliency
Resilience is one of the main challenges that healthcare facilities must tackle today. In order to ensure effective emergency management, the concepts of flexibility and future-proofing represent fundamental aspects to consider in the hospital design process, from the overall building system to the single functional and environmental units.
For example, the Rush University Medical Center in Chicago represents a case study during COVID-19 pandemic. In fact, the hospital can expand both the emergency department capacity and the number of isolation rooms when needed. During ordinary operations, this hospital has around 40 negative pressure rooms that can prevent the spread of potentially infectious diseases in the air. Each environmental unit has a negative pressure with respect to the external corridor, in order to let the air-flow from the corridor into the room, leaving the hospital through the introduction of HEPA filters.
In general, all the interventions that can guarantee a fast reconfiguration are strategic in emergencies, such as:
- the presence of available spaces, empty and support areas among different lots and departments to accommodate expansions, reconfigurations or isolation areas;
- non-sanitary areas easily transformable and to be equipped with low investments. For instance, the underground parking of several hospital in Israel can be converted into a hospital with many beds in wartime or flexible sports facilities ca be reconfigured. Therefore, these areas must be supported by direct internal connections with the rest of the hospital as well as outside for ambulances;
- functional areas that can be easily reconverted, such as common hospital ward that are provided of the proper amount of
technical installations.
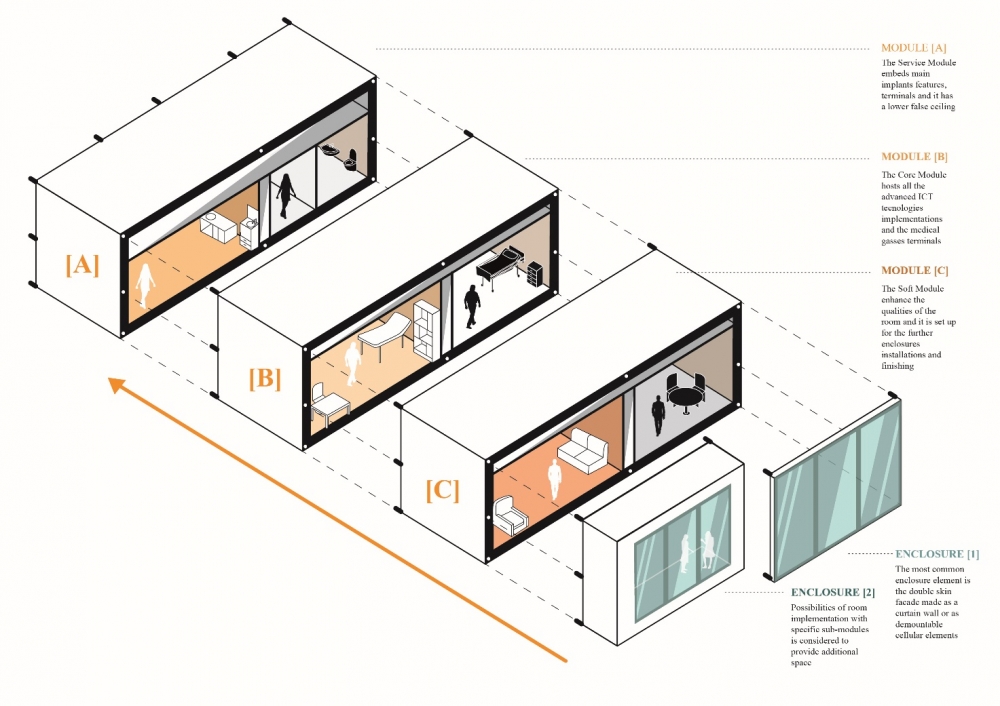
Figure 3. Open Room project developed by Alta Scuola Politecnica, broken down into its three sub-modules. Figure designed by Andrea Brambilla.
4. Functional design and Distribution system
Functional program is fundamental in such complex facilities. In case of emergency, the layout should consider some transversal issues:
- distribution is one of the main aspects to consider within the functional design in relation to emergencies. The access for medical staff must be unique, as well as that one for visitors who are not directed to the emergency department. In case of an infectious emergency, flows that are normally differentiated (public and medical ones), must be able to be further separated, in order to divide the flows of patients with suspected or known infection by other users. In this regard, recognizable signage must effectively indicate temporary changes in
hospital routes;
- the strong relation between the emergency department and infectious wards requires a fast connection for the movement of patients and hospital staff. These spaces should be localized at the same level for short and horizontal connections;
- the presence of storage areas is also required, which in case of infective emergency can host the wide amount of sanitary material, PPE and contaminated waste. There is a need of solutions for the extraordinary placement of corpses in low temperature environments, in close communication with the outdoor driveways for their transport;
- in order to decrease the risk of nosocomial infection's diffusion, all ordinary inpatient wards must maximize the number of single rooms. This can be guaranteed with a set of bed head beams and engineering plant equipment that allow to transform rooms into double rooms in case of hyper flow of patients.
In addition, a resilient hospital design must consider some organizational aspects of both high and low care areas mostly interested by the infectious emergency, such as:
- the results of ICUs as the one of the most affected, so additional filter areas are needed for the dressing/undressing of medical staff. Separated working areas from the main care area are suggested, in order to reduce the workers' exposure and the use of mobile diagnostic equipment;
- the emergency department must at the same time host patients with suspected infection and continue to manage all non-infectious cases, separating them from their entrance. Therefore, two separate entrances are recommended to distinguish sick people through dedicated triage, with separate paths and waiting and treatment spaces. External multiple decontamination areas for ambulances and areas for the preparation of pre-triage tents must be provided;
- the inpatient hotel, which usually welcomes outpatients, relatives or visitors, in emergency conditions must have a flexible configuration that allows to accommodate ordinary and additional medical staff, reducing the infectious risk for their families and ensuring them an effective rest in situations of high work stress. Similarly, it could be transformed to accommodate infectious patients of lower gravity or patient who needs of rehabilitation.
5. User Centeredness
Studies on User-Centered Design highlighted that during all the different phases of the design process, attention must be focused to the physical, psychological and social needs of all users to avoid future disabling situations generated due to COVID-19 or similar overwhelming conditions, as Mosca et al. (2019) stated. This is especially true in hospital environments, where aspects as accessibility, wayfinding and comfort, directly impact on different users during emergencies; in particular, staff shows symptoms of anxiety, depression, insomnia and stress higher than normal within hospital facilities.
In this regard, during the pandemic, some designers developed recharge rooms for hospitals characterized by natural design elements that support medical workers recover from a physically and mentally taxing shift. These spaces were designed to be customized according to the users' needs, such as sounds, sights, and smells. The rooms use bringing the outdoors into built environments - to create spaces with nature out of underused hospital spaces near Intensive Care departments.
Figure 4. SUSThealth tool developed by Politecnico di Milano.
Researches, in fact, have demonstrated that looking at nature can improve recovery patient time and reduce nursing stress levels (Ulrich et al., 2008; Elf et al., 2020).
In addition, Evidence Based Design (EBD) studies demonstrate that the presence of spaces for the physical and psychological well-being is strategic for all users and it also positively influence the work performance of the healthcare staff. Such spaces, in fact, in case of emergency, could guarantee users environments to relax from psychological stress and daily pressures. They can be both areas inside the structure - close to the functional areas - or green areas of the hospital (i.e. garden and terraces), preferably with a variety of spaces, different seats and isolation points to ensure user's privacy.
6. Healthcare Territorial Network for Health Prevention and Promotion
The synergy between territorial services and healthcare organizations plays a crucial role for health promotion. In particular, the adoption of Hub & Spoke model could turn out particularly efficient in cases of high emergencies, avoiding the overflow of users in the hospital thanks to health home care management or low and medium-care facilities (Mauri, 2015).
The community health centers in the territory along with the primary care services and triage activities could ensure a better management of low and medium-care services, as well as to favor the use of smart diagnostics and to support the outpatients management on the territory.
This capillary model encourages access to care for the population, reducing the patients' transfer, decreasing the overcrowding of the emergency departments, and minimizing hospital-based cross-contamination among users and healthcare staff. These healthcare facilities should be configured as integrated hub between healthcare professionals and health and social services. In addition, the use and application of healthcare devices for the smart hospital, as well as telemedicine programs, can easily support and strengthen the health network and the monitoring of the users' health status, even in the presence of healthcare emergencies.
7. Patient Safety and Quality Improvement
It is well-known that healthcare organizations regularly give rise to protocols for risk control and patient safety in hospital settings. In particular, the healthcare leadership needs to reorganize the users' behaviors and healthcare protocols in line with the best practices for the COVID-19 control. Hospital design should give rise to physical environments that support providers to act in a professional, trustful and respectful manner for all the community.
Facility design affects how people work, and what processes, systems and technologies they will require to support the functioning of a learning work environment. It is necessary to take into consideration design strategies aimed at responding to possible emergencies and medical needs for guaranteeing patient safety. For example, among them, several healthcare facilities have included visual cues for visitors and users for highlighting the proximity of risk functional areas and infectious impatient wards. Others have adopted protocols for bringing healthcare devices and materials, as well as the medical waste, through dedicated elevators in an attempt to minimize cross-contamination.
Moreover, for guaranteeing regular disinfection activities, some hospitals adopted spaces called "pods" for low-acuity patients. They were designed to reduce possible risk of infection by separating the patient from the equipment to be cleaned, thus reducing the possibility of contaminating them (Marsilio and Prenestini, 2020).
Many hospitals adopted strategies, such as adhesive tape on the floor, signage and signs boards on door used for annotations with special markers, intentionally positioned. Stations for accessing the PPE were provided in strategic positions, which in turn influenced the way and the place in which the hospital staff used the equipment.
Clear and immediate visual devices, wayfinding strategies and design-nudges can help to mitigate the transmission of infections by clearly defining risky areas, creating mental anchors for specific activities (Jamshidi and Pati, 2020) and consequently reducing mental fatigue and helping to align the behavior with the protocols to be followed.
8. HVAC and Indoor Air Quality
It is well-known that indoor air quality (IAQ) plays a direct or indirect leading role in prevention, especially in environments with vulnerable users. The quality of the air depends not only on the outdoor air but also on the presence of indoor sources that emit pollutants that can affect its composition (Gola et al., 2019). It is therefore necessary to ensure adequate air exchanges in all the hospital settings through mechanical and, where possible, mixed ventilation.
To ensure efficient management in case of emergency, such as infectious epidemics the ventilation systems have a strategic role, but its functioning must be able to respond to different healthcare needs, in all the conditionsand especially in emergencies where air could be a possible means of infection diffusions (Correia et al., 2020; Li et al., 2007). The heating, ventilation, and air conditioning (HVAC) must be flexible and their operation must be able to be modified in terms of the air used, from recirculation to all-air systems, and pressure, from positive to negative. In addition, their regular and constant maintenance, cleaning and disinfection also become strategic through the use of innovative materials. As a consequence, new generation systems must be designed with solutions that guarantee easy inspection, and the possibility of intervention (Joppolo and Romano, 2017).
9. Finishing Materials and Furniture
Healthcare Acquired Infections (HAIs) have a relevant role in the light of the management of the COVID pandemic. In synergy with monitoring and risk management activities, it is necessary to use high-performance, long-lasting and easy to clean materials in relation to the medical needs. In particular, innovative materials must be introduced to reduce the bacterial (and viral) load on the finishing surfaces (van Doremalen et al., 2020) among which also eco-active ones and photocatalytic paints, as well as characterized by high performances and flexibility-in-use. It is necessary to investigate and take into consideration, also, solutions used in emergency contexts such as, for example, washable textile materials. Their application could be extended in many healthcare areas for social distancing, and which in case of need can be easily clean and replaced, and/or removed for guaranteeing the adaptability and resilience of the spaces (Zanelli et al., 2020).
Together with the application of best practices of ventilation, the cleaning products must be defined in relation to the furnishings and finishing materials considering each surface characteristics (Kampf et al., 2020). In addition, several detergents have chemical compositions that kill the bacterial and antiviral load but, at the same time, they can present volatile organic compounds (VOCs) toxic to humans, and require paying attention to environmental sustainability.
10. Healthcare Digital Innovation
The new digital technologies can support the patients' treatment and care processes both in the hospital and on the territorial healthcare network, also in case of emergency. In fact, the continuous control of the health status and vital parameters through IT systems, such as smartphone or wearable devices, can guarantee a better management of hospitalization, and consequently an efficient organization
of hospital settings.
Moreover, the modular planning and forecasting of the occupation of ICUs and ordinary beds, both in the same hospital and within the territorial hospital network, can support the possible directing of the ambulances to the more appropriate healthcare facility. In addition, the constant monitoring and technological advancement allows the use of some electro-medical equipment remotely, decreasing the contacts between (infected) patients and hospital staff, and guaranteeing an overall control and a more efficient use of the resources.
As well as the use of sensors and devices through the Internet of Things allows the hospital to guarantee an experience for each user, monitoring the degree of comfort and satisfaction.
In the close future all medical procedures that can be treated without physical presence, will be carried out through digital systems and healthcare organizations will also be able to better manage patients' clinical information and therefore users at risk will be more protected through tailored medical paths. Nowadays more than ever, digital system should be integrated with structural innovations that would enable access to health services worldwide and in different condition guaranteeing safety and security to patients and health workers.
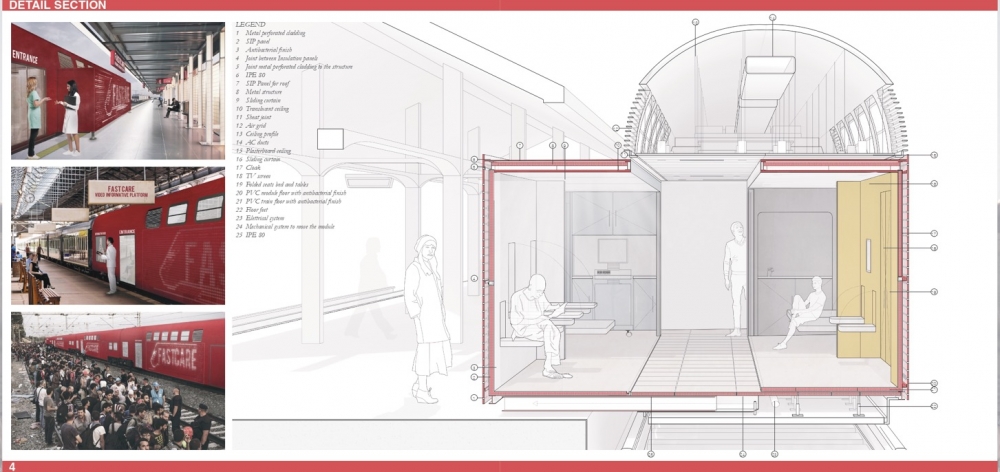
Figure 5. Fast care, designed by Politecnico di Milano.
Future perspectives
COVID-19 pandemic has accelerated all those processes of innovation already activated. In the same way, the hospital, which in the face of this gradual process of dematerialization and relocation of "softer" clinical diagnostic activities, reaffirms itself as a center of the highest specialty for the treatment and care of acute patients, for high-level clinical and experimental research, for diagnostics and more complex operations.
For example, antimicrobial resistance has been recently highlighted by several institutions due to the mis-use and/or overuse of antibiotics in human medicine, specific facilities for infectious diseases treatment and containments emerged (Lanbeck et al., 2016). The pandemic highlighted that a post-antibiotic era can be very difficult to tackle and the role of built environment is of increasing importance. Indeed, due to the high diffusion and infectious rates of COVID and in the waiting time to reliable drugs or specific vaccinations, the pandemic containment has been mainly performed through physical and social tool such as the confinement practices and hand washing prescriptions. Indeed, the hospital will have to increasingly reflect on its role of health promotion and protection, especially towards the most fragile users.
Considering all those issues, it is essential to promote multidisciplinary actions and monitoring programs for quality improvement through evidence-based evaluation tools in order to develop a new design for the hospital of the near future. Further multidisciplinary researches is encouraged to validate the presented strategies in case studies and in empirical settings.
The Decalogue of strategies aims to briefly indicate the key strategies to be considered in the design of new resilient hospitals and in the re-functionalization of existing structures.
Acknowledgements
We thank prof. Paul Barach, Arch. Erica Isa Mosca and Dr. Alessandro Morganti for their support in the research activity and useful considerations and suggestions.
References
AIA. AIA's COVID-19 Task Force Creates Design Guide to Retrofit Buildings for Alternative Care. ArchDaily, 2020. Available from: https://www.archdaily.com/937331/aias-covid-19-task-force-creates-design-guide-to-retrofit-buildingsfor-alternative-care [Accessed: 21st June 2020]
BARACH, P., FISHER, S.D., ADAMS, M.J., et al. Disruption of healthcare: Will the COVID pandemic worsen non-COVID outcomes and disease outbreaks? Progress in Pediatric Cardiology. 2020; 101254. doi:10.1016/j.ppedcard.2020.101254
CAPOLONGO, S., COCINA, G., PERETTI, G., POLLO, R., GOLA, M. Horizontality and verticality in architectures for health. TECHNE - Journal of Technology for Architecture and Environment. 2019;17: 152-160. Available from: doi:10.13128/Techne-24028
CAPOLONGO, S., GOLA, M., BRAMBILLA, A., MORGANTI, A., MOSCA, E.I., BARACH, P. COVID-19 and healthcare facilities: A decalogue of design strategies for resilient hospitals. Acta Biomedica 2020; 91:50-60. Doi:10.23750/abm.v91i9-S.10117
Capolongo Stefano. Architecture for Flexibility in Healthcare. Milan, Franco Angeli, 2012.
CORREIA, G., RODRIGUES, L., GAMEIRO DA SILVA, M., GONÇALVES, T. Airborne route and bad use of ventilation systems as nonnegligible factors in SARS-CoV-2 transmission. Medical Hypotheses. 2020;141: 109781. doi:10.1016/j.mehy.2020.109781
DELL'OVO, M., CAPOLONGO, S., OPPIO, A. Combining spatial analysis with MCDA for the siting of healthcare facilities. Land Use Policy. 2018;76: 634-644. Available from: doi:10.1016/j.landusepol.2018.02.044
ELF, M., ANÅKER, A., MARCHESCHI, E., SIGURJÓNSSON, Á., ULRICH, R.S. The built environment and its impact on health outcomes and experiences of patients, significant others and staff-A protocol for a systematic review. Nursing Open. 2020; doi:10.1002/nop2.452
GOLA, M., SETTIMO, G., CAPOLONGO, S. Indoor Air Quality in Inpatient Environments: A Systematic Review on Factors that Influence Chemical Pollution in Inpatient Wards. Journal of Healthcare Engineering. 2019;2019: 1-20. doi:10.1155/2019/8358306
JAMSHIDI, S., PATI, D. A Narrative Review of Theories of Wayfinding Within the Interior Environment. HERD: Health Environments Research & Design Journal. 2020; 193758672093227. doi:10.1177/1937586720932276
JOPPOLO, C.M., ROMANO, F. HVAC System Design in Healthcare Facilities and Control of Aerosol Contaminants: Issues, Tools, and Experiments. In: Capolongo S, Settimo G, Gola M (eds.) Indoor Air Quality in Healthcare Facilities. Cham: Springer International Publishing; 2017. p. 83-94. doi:10.1007/978-3-319-49160-8_8
KAMPF, G., TODT, D., PFAENDER, S., STEINMANN, E. Persistence of coronaviruses on inanimate surfaces and their inactivation with biocidal agents. Journal of Hospital Infection. 2020;104(3): 246-251. doi:10.1016/j.jhin.2020.01.022
LANBECK, P., RAGNARSON TENNVALL, G., RESMAN, F. A cost analysis of introducing an infectious disease specialist-guided antimicrobial stewardship in an area with relatively low prevalence of antimicrobial resistance. BMC Health Services Research. 2016;16(1): 311. doi:10.1186/s12913-016-1565-5
LI, Y., LEUNG, G.M., TANG, J.W., et al. Role of ventilation in airborne transmission of infectious agents in the built environment? A multidisciplinary systematic review. Indoor Air. 2007;17(1): 2-18. doi:10.1111/j.1600-0668.2006.00445.x
MARSILIO, M., PRENESTINI, A. Making it happen: Challenges and transformations in health care processes, people management, and decision-making. Health Services Management Research. 2020;33(2): 53-54. doi:10.1177/0951484820906314
MAURI, M. The future of the hospital and the structures of the NHS. TECHNE - Journal of Technology for Architecture and Environment. 2015; 27-34. doi:10.13128/Techne-16100
MIEDEMA, E., LINDAHL, G., ELF, M. Conceptualizing Health Promotion in Relation to Outpatient Healthcare Building proposed in the commentary Design: A Scoping Review. HERD: Health Environments Research & Design Journal. 2019; 12(1): 69-86. Available from: doi:10.1177/1937586718796651
MOSCA, E.I., HERSSENS, J., REBECCHI, A., CAPOLONGO, S. Inspiring architects in the application of design for all: knowledge transfer methods and tools. Journal of Accessibility and Design for All. 2019;9(1). doi:10.17411/jacces.v9i1.147
ULRICH, R.S., ZIMRING, C., ZHU, X., et al. A Review of the Research Literature on Evidence-Based Healthcare Design. HERD: Health Environments Research & Design Journal. 2008;1(3): 61-125. doi:10.1177/193758670800100306
VAN DOREMALEN, N., BUSHMAKER, T., MORRIS, D.H., et al. Aerosol and Surface Stability of SARS-CoV-2 as Compared with SARS-CoV-1. New England Journal of Medicine. 2020; 382(16): 1564-1567. doi:10.1056/NEJMc2004973
VV.AA. Impact of the Covid-19 pandemic on healthcare systems? Deloitte France, 2020. Available from: https://www2.deloitte.com/fr/fr/pages/covid-insights/articles/impact-covid19-healthcare-systems.html [Accessed: 18th June 2020]
WHO. Hospital Readiness Checklist for COVID-19. World Health Organization Regional Office, 2020. Available from: https://www.euro.who.int/__data/assets/pdf_file/0010/430210/Hospital-Readiness-Checklist.pdf
ZANELLI, A., CAMPIOLI, A., MONTICELLI, C., VISCUSO, S., GIABARDO, G. Novel Textile-Based Solutions of Emergency Shelters: Case Studies and Field Tests of S(P)EEDKITS Project. In: Aste N, Della Torre S, Talamo C, Adhikari RS, Rossi C (eds.) Innovative Models for Sustainable Development in Emerging African Countries. Cham: Springer International Publishing; 2020. p. 111-122. doi:10.1007/978-3-030-33323-2_10
Stefano Capolongo: Professor in hospital design at Politecnico di Milano (Italy) and director of the Department of Architecture, Built environment and Construction engineering. Currently he is the coordinator of the European chapter of the International Academy for Design and Health and President of the Urban Health section of the European Public Health Association, as well as the coordinator of the Design and Health LAB at Politecnico di Milano. stefano.capolongo@polimi.it
Andrea Brambilla: Architect and PhD candidate at Politecnico di Milano (Italy); in addition he took part to the program IDEA League Visiting PhD at Chalmers University of Technology (Sweden). He is one of the member of the Design and Health LAB at Politecnico di Milano. andrea1.brambilla@polimi.it
Marco Gola: Architect, PhD and Research fellow at Politecnico di Milano (Italy). He is one of the member of the Design and Health LAB at Politecnico di Milano and currently he is the vice-secretary of CNETO, the Italian National Center for Hospital Design, Construction and Technology. marco.gola@polimi.it
Share




Send by e-mail: